□ 서 론
- 로봇수술은 2005년 식품의약품안전청의 승인을 받고, 건강보험 비급여 항목으로 등재되어비뇨기과, 외과, 산부인과, 흉부외과 등 다양한 분야에서 활발히 활용되고 있다.
- 로봇수술은 개복수술에 비하여 감염 위험이 낮고, 국소부위를 절개함으로 환자의 고통과 출혈이 적고 회복속도가 빠르고, 수술 후 흉터가 작다는 등의 장점이 있다.
- 그러나 수술팀의 숙련도와 학습시간에 따라 수술결과의 편차가 크기 때문에 일정 수준의 학습곡선을 극복하여야 한다. 또한 촉감 정보의 제약으로 시술부위 주변의 천공 및 조직손상의 부작용이 빈번히 보고되고 있다.
- 국내에서는 로봇수술이 기존 기술에 비하여 비용 효과적이지 않다는 지적과 함께 안전성에 대한 의문들이 전문가들에 의하여 제기되고 있다.
- 본 연구에서는 국내 다빈도 시술 5개 질환(전립선암, 신장암, 직장암, 위암, 갑상선암)에 대한 국내 코호트자료 분석과 체계적 문헌고찰을 통하여 로봇수술의 안전성과 유효성을 검토하고자 한다.
- 본 연구의 결과는 임상에서 로봇수술 관련 의사결정시 유용한 근거자료로 활용될 수 있고, 로봇수술 관련 국가 건강보험 정책수립 시 기초자료로 활용될 수 있을 것으로 기대된다.
□ 연구방법
Ⅰ. 현황 연구
1. 로봇수술 환자 현황
- 보건복지부 협조를 통해 2005년 9월부터 2011년 12월 사이 국내에서 로봇수술을 시술받은 전체 대상자 20,944명에 대한 병원자료의 주민등록번호를 활용하여 통계청 사망원인 자료와 2008년 1월 1일부터 2012년 12월 31일 사이에 발생한 청구자료를 연계하여 코호트 자료 를 구축하였다.
- 최종 분석대상자는 코호트 자료 중 2011년 로봇수술을 시술받은 전립선암, 갑상선암, 직장암, 위암, 신장암 환자이다.
2. 분석내용
- 질환별 로봇수술 연구대상자들의 기본특성(성별 및 연령분포)을 파악하고, 임상전문가들의 자문을 통해 청구 자료로 확인할 수 있는 유의미한 결과지표(사망, 입원일수, ICU 재입원, 수혈, 마취 등)에 대하여 분석하였다.
Ⅱ. 체계적 문헌고찰
1. 전립선암
- 전립선암에 때한 로봇수술의 안전성 및 유효성 평가는 기존에 출판된 체계적 문헌고찰을 활용하는 의료기술평가방법론을 수행하였다.
- 질평가는 R-AMSTAR를 이용하였으며, 질평가 결과 “A등급 이상”의 2010년 이후에 출판된 체계적 문헌고찰을 최상의 사용 가능한 근거로 채택하였다.
- 채택된 체계적 문헌 고찰의 검색기간 1년 이전부터 현재까지 출판된 RCT와 비교관찰연구를 추가로 선택하고, 국내 데이터베이스에서 검색된 비교관찰연구 이상의 일차연구들의 치료효과크기를 추출하여 각 관심 의료결과에 대한 전체 메타분석을 수행하였다.
2. 신장암, 직장암, 위암, 갑상선암
- 신장암, 직장암, 위암, 갑상선암에 대하여 체계적 문헌고찰을 수행하였다.
- 사용한 database
· 사용한 국외 database는 OvidMedline, Ovid EMBASE, CENTRAL이었다. 국내 database는 KoreaMed, KMbase, KISS, RISS, KisTi이었다.
|
선택기준 |
배제기준 |
|
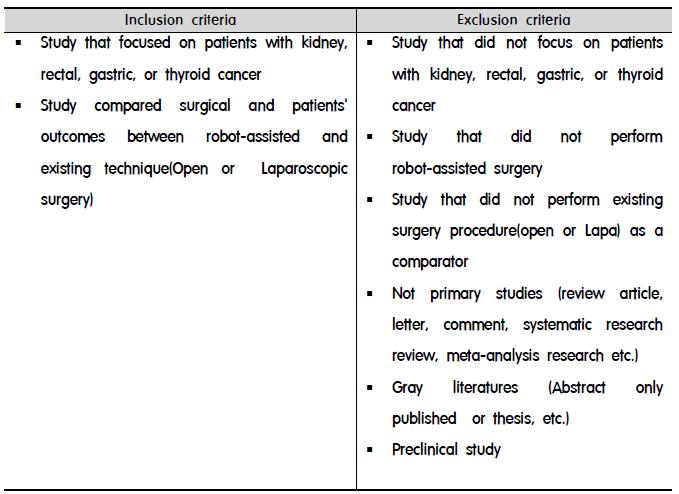
․ 기 정의한 연구대상을 만족하는 경우
․ 로봇수술을 시행하고 비교치료법으로 복강경(또는 내시경) 수술 또는 Open surgery를시행한 연구
․ 로봇수술과 비교수술(복강경, 내시경 수술 또는 Open surgery) 간의 치료성과를 비교하여 제시한 연구 |
․ 기 정의한 연구대상을 연구대상으로 하지 않은 연구
․ 로봇수술을 시행하지 않은 연구
․ 비교 치료법으로 복강경, 내시경 수술 또는 Open surgery를 실시하지 않은 연구
․ 로봇수술과 비교 치료법(복강경, 내시경 수술 또는 Open surgery) 간 치료 성과를 보고하지 않은 연구
․ 원저가 아닌 연구(종설, letter, comment, 체계적 문헌고찰, meta-analysis 연구 등)
․ 회색문헌(초록만 발표된 연구, 학위논문 등 )
․ 인간 대상 연구가 아닌 경우(동물 또는 전임상단계) |
- 문헌의 질평가
· 최종 선택된 문헌에 대하여 비무작위연구의 경우 MINORS를 활용하여 질평가를 수행하였고, 전향적 무작위비교임상연구의 경우 Cochrane의 RoB를 활용하여 질평가를 수행하였다.
- 주요 자료추출 내용
· 주요 자료추출 내용은 연구방법, 연구대상, 로봇수술 관련 자료, 비교수술법 관련 자료, 연구결과 등이다.
- 자료분석
· 양적 분석(quantitative analysis)이 가능할 경우 메타분석을 수행하였으며, 양적 분석이 어려운 경우 질적 검토(qualitative review)를 수행하였다.
Ⅲ. 연구결과 설명회
- 목적
· 전립선암, 신장암, 직장암, 위암, 갑상선암의 5개 암종에 대한 로봇수술의 안전성과 유효성 연구결과를 관련 연구자 및 보건의료정책 의사결정자 등과 공유함으로써 연구결과를 확산하고 연구결과에 대한 의견수렴을 통하여 연구결과의 신뢰도 및 완성도를 제고하고자 함.
· 일 시 : 2013년 12월 18일(목), 14:00∼18:10
· 장 소 : 한국보건의료연구원, 컨퍼런스 룸
· 주요 참석자 : 관련 주요 12개 학회, 보건복지부 관련 부서, 관련 기관 연구자, 관련 임상 연구자, Intuitive Surgical 한국지부 등 83명
□ 연구결과
Ⅰ. 전립선암
1) Robot vs Open
- 안전성 중 부작용발생위험은 1) 방광목구축 2) 주변장기손상 3) 폐색전증에서 로봇수술이 개복수술에 비해 발생위험이 낮은 것으로 나타났다.
- 유효성은 수술관련 의료결과에서, 1) 수혈발생이 적고2) 재원일수가 더 짧았으나, 3) 수술시간은 로봇수술이 개복수술보다 더 긴 것으로 나타났다. 하지만 재원일수와 수술시간의 경우 이질성이 높아 결론을 내리기 어려웠다. 기능적 의료결과에서 1) 12개월 시점의 요실금발생위험은 로봇수술이 개복수술에 비해 발생위험이 낮은 것으로 나타났으며 2) 성기능회복율은 로봇수술이 개복수술보다 높은 것으로 나타났다. 종양학적의료결과에서 1) 절제면양성률은 발생위험의 차이가 없는 것으로 나타났으나 2) 생화학적 재발율은 로봇수술이 개복수술에 비하여 발생위험이 낮은 것으로 나타났다.
2) Robot vs Lapa
- 안전성 중 1) 개복수술로의 전환률에서는 두 군간에 차이가 없는 것으로 나타났으나, 부작용 발생위험의 경우 2) 방광목 구축 3) 주변장기손상에서 로봇수술이 복강경수술에 비해발생위험이 더 낮은 것으로 나타났다.
- 유효성 항목 중 수술 관련 의료 결과에서 1) 수혈의 경우 로봇수술이 복강경수술에 비하여 발생위험이 낮았고 2) 수술시간이 짧았으나 이질성이 높아 결론을 내리기 어려웠다. 3)재원일수는 역시 전체적으로는 로봇이 짧은 경향을 보였으나, 국가별로 수행하였을 때 asia-pacific 지역은 차이가 없는 것으로 나타났다. 하지만 이질성이 높아 결론을 내리기 어려웠다. 기능적 의료결과에서 1) 12개월 시점의 요실금 발생위험은 차이가 없었으나 2) 성기능 회복율은 로봇수술이 복강경수술에 비해 유의하게 높은 것으로 나타났다. 종양학적의료결과에서 1) 절제면양성률은 두 군간에 발생위험의 차이가 없는 것으로 나타났으나 2)생화학적재발은 전체적으로 로봇수술이 복강경에 비하여 발생위험이 낮은 것으로 나타났다.
Ⅱ. 신장암
1) Robot vs Open
- 부분 신절제술에서 수술시간과 온허혈시간이 개복수술에 우호적인 경향을 보였으나, 재원기간은 로봇수술이 짧은 것으로 나타났다. 그러나 문헌의 양이 적고 대부분이 후향적 관찰연구로 문헌의 질이 낮은 것으로 평가되었다.
2) Robot vs Lapa
- 로봇 부분 신절제술의 경우 1) 개복수술 및 근치적 신적출술로의 전환률이 낮고 2) 신장기능보존의 매개변수인 추정 사구체 여과율에 있어서 유효한 것으로 나타났다. 3) 또한 재원기간도 복강경수술에 비하여 짧은 것으로 나타났으나 포함된 연구의 대부분이 후향적 관찰연구로 문헌의 질이 낮은 것으로 나타났다.
Ⅲ. 직장암
1) Robot vs Open
- 안전성 결과 지표에서는 요정체에서 로봇수술이 개복수술에 비해 요정체 발생이 낮게 나타났다.
- 유효성 결과 지표 중 유의한 결과는 로봇수술에서 출혈량이 적었으며, 연동식 시작시간과 가스 배출 시간이 빨랐다. 반면 수술시간은 로봇수술이 개복수술보다 길었다.
2) Robot vs Lapa
- 안전성 결과 지표에서는 open 수술로의 전환에서 로봇수술이 복강경 수술에 비해 open 수술로의 전환율이 낮게 나타났다.
- 유효성 결과 지표에서는 로봇수술에서 가스배출 시작 시간이 복강경 수술보다 짧았다. 하지만 로봇수술의 수술시간은 복강경수술에 비하여 길었다.
Ⅳ. 위암
1) Robot vs Open
- 로봇수술 군에서 재원 기간이 개복수술군보다 짧은 것으로 나타났다. 수술 과정 중 발생하는 출혈량도 로봇수술 군이 개복수술 군에 비해 작았다. 그러나 수술시간은 로봇수술이 개복수술보다 긴 것으로 나타났다.
2) Robot vs Lapa
- 로봇수술군의 재원기간이 짧은 것으로 나타났고, 출혈량도 적었으며, 연동식 시작시간도 빠른 것으로 나타났다. 반면 로봇수술의 수술시간은 복강경수술에 비하여 길었다.
Ⅴ. 갑상선암
1) Robot vs Open
- 안전성 지표에서 일시적 성대마비 발생위험이 로봇수술 군에서 개경수술 군보다 높은 것으로 나타났다. 유효성 지표에서는 출혈량이 개경수술 군보다 로봇수술 군에서 더 적은 것으로 분석 되었고, 수술 3개월 후 미용만족도가 개경수술 군 보다 로봇수술 군에서 더 높은 것으로 나타났다.
2) Robot vs Endo
- 안전성 지표 중 일시적 부갑상선기능저하증 발생위험이 로봇수술 군에서 내시경수술 군보다 높은 것으로 분석되었다. 유효성 지표에서는 두 군 간에 통계적으로 유의미한 차이가 보이는 지표가 없는 것으로 나타났다.
□ 연구의 의의 및 제한점
1. 연구의 의의
- 본 연구결과는 로봇수술 관련 건강보험 정책 수립시 유용한 근거자료로 활용 가능하다.
- 임상에서 수술법 선택시 유용한 근거자료로 활용 가능하다.
2. 제한점
- 신장암, 직장암, 위암, 갑상선암에서의 로봇수술의 치료성과를 평가하기에는 포함된 문헌의 수가 충분하지 않았으며 전향적 연구가 부족하여 근거수준이 낮았다. 또한 종양학적 치료성과를 평가하기에는 문헌의 추적관찰 기간이 충분하지 않았다. 따라서 질환별로 충분한 문헌의 확보가 가능한 시점에서 추가연구를 수행하여야 할 것이다.
□ 결론 및 정책제언
1. 전립선암
- 로봇수술이 기존수술법에 비해 기능적 결과에 있어서 더 좋은 치료성과를 보이고 있다는 것은 알려진 결과이다. 그러나 종양학적 결과에 있어서는 장기 추적된 연구결과가 없어 결론을 도출하기에는 근거가 부족하였다. 따라서 추가 연구가 필요하다. 또한 로봇수술에 대한 건강보험 정책지원을 위하여 경제성 평가 연구의 수행이 필요하다.
2. 신장암
- 부분 신절제술에서 로봇수술의 치료성과를 평가하기에는 결과변수별로 문헌의 수가 충분하지 않은 경우가 많았으며, 전반적인 문헌의 질이 낮아 결론을 도출하기에는 근거가 부족하였다. 따라서 로봇수술의 치료성과를 평가하기 위해서는 장기적 관점에서의 무작위배정임상연구가 필요하다.
3. 직장암
- 로봇수술은 복강경수술 대비 개복수술로의 전환율이 낮았으며, Urinary function과 Sexualfunction에서 로봇수술의 치료성과가 복강경수술에 비하여 좋은 치료성과를 보이고 있다. 따라서 직장암에서의 로봇수술의 활용도는 증가할 것으로 예측된다. 이를 위해서는 전향적 무작위배정 임상연구를 통하여 로봇수술의 치료성과를 객관적으로 평가하여야 할 것다.
4. 위암
- 위암에서 로봇수술과 복강경수술의 치료성과 비교시 사망률과 합병증 발생률에는 차이가 없고 로봇수술이 재원기간을 약간 줄였다.
- 위암에서 로봇수술이 시행 초기단계임을 고려할 때 학습곡선을 극복한 후의 전향적 무작위배정 임상연구를 통항 치료성과 평가연구의 수행이 필요하다.
5. 갑상선암
- 갑상선암에서 로봇수술은 최소침습수술이 아닌 remote access 수술법으로 간주해야 하므로, 다른 종양에서처럼 개경수술에 비해 빠른 회복, 적은 통증 등으로 환자의 삶의 질을 높일 수 있다는 식의 접근은 적절하지 않다. 또한 상완총신경손상 같이, 드물지만 로봇수술의 적용으로 인해 새롭게 생겨난 합병증이 있음도 유의하여야 한다.
- 로봇수술의 치료성과에 대한 근거부족과 개경수술에 비해 수술비가 고가임을 고려하여 갑상선암에서 로봇수술이 적절한가에 대한 사회적 합의가 필요하다.
- 장기적 관점에서 전향적 무작위배정 임상연구를 통한 임상적 유효성과 안전성 평가의 수행이 필요하다.
Clinical Effectiveness and Safety of Robotic Surgery
□ Introduction
- In Korea, robot-assisted surgery uncovered by national health insurance has been often utilized in various
areas such as urology, general surgery, obstetrics, gynecology, and thoracic surgery since it received Ministry
of Food and Drug Safety (MFDS) approval in 2005.
- Compared with conventional open surgery, the benefits of robot-assisted surgery are as follows: low risk of
infection, preventing excessive blood loss, minimized surgical related scars, and recovery faster for small
incision.
- However, as there is large variation in surgical outcomes depending on the individual surgeon's rate of learning
so that those who want to use the technology for their patients should overcome the learning curve. In addition,
because of tactile limited, the side effects, such as perforations or organ injury, have been frequently reported.
- Experts in Korea have raised concerns about safety of the robot-assisted surgery procedures, pointing out that
it is not cost-effective compared to existing technologies.
- This study is intended to evaluate safety and effectiveness of the robot-assisted surgery to five kinds of cancer
disease (prostate cancer, kidney cancer, rectal cancer, gastric cancer, and thyroid cancer) which are the most
frequently performed in Korea, through domestic cohort data analysis and systematic literature review.
- The results of this study might be used as valuable resources in the clinical decision-making related to robot-
assisted surgeries, and it is also expected to be used as primary information for establishing the relevant
national health care policy.
□ Method
Ⅰ. Research for Current Status of robot-assisted surgeries in Korea
1. Current status
- In cooperation with Ministry of Health and Welfare and tertiary hospitals, we received whole hospital
registries for 20,944 subjects through robot-assisted surgeries between September, 2005 and December, 2011
in Korea, and then linked up the data with national cause of deaths database of Statistics Korea, matching on
identification numbers of the subjects. After that we linked up again the data set with the Health Insurance
Review & Assessment Services's health insurance claims data between January 1, 2008, and December 31,
2012 and determined it as our final cohort data set for the study.
- Final subjects in the analysis using the cohort data only were chosen patients who received robotic surgical
procedures for tumor in prostate, kidney, rectum, stomach, or thyroid in 2011.
2. Analysis
- We explored baseline characteristics of the subjects included the final data set, such as gender and age
distribution, and then analyzed it by important indicators(mortality, hospital stay, ICU readmission, blood
transfusion, anesthesia, etc.) based on consultation with clinical experts.
Ⅱ. Systematic Review of Literatures
1. Prostate cancer
- We performed a systematic review using existing systematic reviews (SR) to investigate clinical effectiveness
and safety of robot-assisted surgery for prostate cancer, compared with open or laparoscopic surgery.
- R-AMSTAR was used to assess quality of the existing SRs and, as a result, two HTA reports published in
2011 and 2012, respectively, were selected as a available evidence with the best quality.
- RCT and comparative observational studies carried out on abroad and published from 2009 to August 2013 and
domestic comparative studies were additionally included in the process. All meta-analyzes were performed
on each of interested medical outcome, extracting the treatment effect size of both primary and secondary
studies included.
2. Kidney cancer, rectal cancer, gastric cancer, thyroid cancer
- Full systematic review process was carried out on kidney cancer, rectal cancer, gastric cancer, and thyroid
cancer, respectively.
- Database
· Ovid MEDLINE, Ovid Embase, and CENTRAL were primarily used to search related literatures. Domestic
databases (Korea Med, KMbase, Kiss, Riss, KisTi) were also used to search studies conducted in
domestic area.
- Inclusion / exclusion criteria
- Quality assessment of the literatures included in the process
· MINORS and RoB of Cochrane was used in order to assess quality of observational studies and prospective
randomized controlled studies, respectively.
- Data extraction
· Method, target population, information relating to robotic and comparative technique, and important outcomes
were extracted using a standardized data extraction form.
- Data analysis
· Meta analysis was performed if the quantitative analysis is applicable, but if not, just brief descriptions were
presented.
Ⅲ. Presentation meeting
- Objective
· The meeting aimed to strengthen reliability and completeness of our study's results and spread our findings
to related researchers and health care policy decision-makers, by sharing the study's results and hearing
publically comments and suggestions from the participants.
· When : December 18, 2013 (Thursday), 14:00∼18:10
· Where : National Evidence based Health care Collaborating Agency, Conference Room
· Main Participants : 83 people, including 12 related academic associations, the relevant government
departments in Ministry of Health and Welfare, Intuitive Surgical Korea, related researchers and clinicians.
□ Result
Ⅰ. Prostate Cancer
1) Robot vs Open
- Robotic surgery when compared with open surgery is associated with low risk of complication (bladder neck
contracture, organ injury, pulmonary embolism etc.) and low risk of peri-operative outcome. Also, robotic
surgery is associated with reduction in the length of hospital stay, although there was high degree of
heterogeneity. The risk of functional outcome was higher in robotic surgery compared open surgery. However,
there was no significant difference between robotic and open surgery regarding oncological outcome.
2) Robot vs lapa
- The risk of complication, such as organ injury, major complication in Clavien Dindo classification) was lower
in robotic surgery compared laparoscopic surgery. robotic surgery when compared with laparoscopic surgery
is associated with improvement of functional outcomes. Also, according to subgroup analysis robotic surgery
has low risk of oncological outcomes.
Ⅱ. Kidney Cancer
1) Robot vs open
- In partial nephrectomy, open surgery shows favorable tendency compared with robot-assisted surgery in the
operative time and warm ischemia time (WIT), but the robot-assisted surgery shows a shorter hospital stay.
However, the numbers of literature was limited and most of them were retrospective observational studies,
indicating the quality of evidence was low.
2) Robot vs lapa
- In partial nephrectomy robot-assisted surgery shows 1) lower conversion rate to open surgery and radical
nephrectomy, and 2) favourable estimated glomerular filtration rate (eGFR) that indicate the preservation of renal
function. 3) reduction in the length of hospital stay, compared with laparoscopic surgery. But it is shown that
the quality of evidence is low because most of included studies are retrospective observational studies.
Ⅲ. Rectal Cancer
1) Robot vs open
- Robot-assisted surgery when compared with open surgery was associated with low risk of urinary retention.
- Both time to soft diet and flatus passage were significantly faster in the patients thorough robot-assisted
surgery compared to open surgery, while operation time for robot-assisted surgery was longer than for open
surgery.
2) Robot vs lapa
- Robot-assisted surgery when compared with laparoscopic surgery was associated with low risk of conversion
rate to open surgery.
- Both time to soft diet and flatus passage were faster in the patients thorough robot-assisted surgery compared
to laparoscopic surgery. However, there were no significant differences between those outcomes of both robot-
assisted and laparoscopic surgery. And operation time for robot-assisted surgery was longer than those of
laparoscopic surgery.
Ⅳ. Gastric Cancer
1) Robot vs Open
- The postoperative hospital stay in the RAG(Robot-Assisted Gastrectomy) group was shorter than in the OG
(Open Gastrectomy) group. The estimated blood loss was more reduced in the RAG(Robot-Assisted
Gastrectomy) group as compared with the OG(Open Gastrectomy) group. However, the operative time was
longer in RAG(Robot-Assisted Gastrectomy) group than in the OG(Open Gastrectomy) group.
2) Robot vs Lapa
- The RAG(Robot-Assisted Gastrectomy) group showed shorter postoperative hospital stay, less estimated
blood loss and starting time faster for soft diet, but the operative time in the RAG(Robot-Assisted Gastrectomy)
group was longer than in the LAG(Laparoscopic-Assisted Gastrectomy) group.
Ⅴ. Thyroid Cancer
1) Robot vs open
- Regarding safety outcomes, robot-assisted thyroidectomy when compared with open thyroidectomy was
associated with high risk of temporary vocal cord palsy. Volume of estimated blood loss, one of the outcomes
evaluated effectiveness of the surgery, was smaller the robot-assisted thyroidectomy than the open
thyroidectomy and also the robot-assisted group were more satisfied with post-operative cosmetic results at
three months after the surgery, comparing with open surgery group.
2) Robot vs Endo
- Regarding safety outcomes, robot-assisted thyroidectomy when compared with endoscopic thyroidectomy
was associated with high risk of temporary hypoparathyroidism. On the other hands, there were no significant
differences between robot-assisted thyroidectomy and open thyroidectomy regarding effectiveness outcomes.
□ Strength and Limitation of the Study
1. Strength
- The findings of this study might be useful when establishing a health insurance policy related robot-assisted
surgery.
- It would be a good resource to related clinicians and patients when they build treatment strategy up .
2. Limitation
- In kidney, rectal, gastric, and thyroid cancer, the low quantity and poor quality of evidence were the major
limitation on this study because of no prospective randomized controlled studies and lack of the absolute
number of related literatures. Many studies in our review were reported insufficient follow-up period so that
much of data from the studies was unsuitable for evaluation of oncological outcomes.
□ Conclusions and Policy Recommendations
1. Prostate Cancer
- Although there was high degree of heterogeneity, this study presented that robot surgery is superior in terms of
safety, peri-operative outcome, functional outcome and oncological outcome compare the laparoscopic or
open surgery. However it was not sufficient to support long term outcomes. Therefore, well designed long term
follow-up prospective studies and cost effectiveness study are needed.
2. Kidney Cancer
- In order to evaluate the treatment effect of robotic surgery in partial nephrectomy, the numbers of literature were
not sufficient, and the level of evidence is not high for evaluating treatment effects. Therefore, in order to evaluate
the outcomes of robotic surgery, well designed randomized clinical study is required in the future.
3. Rectal Cancer
- The conversion rate to open surgery showed significantly low in robotic surgery. Recently, urinary function and
sexual function after robotic surgery were more improved. Thus, it is expected that robotic surgery in rectal
cancer patients is more increased. So this result needs to be verified by large prospective randomized clinical
trials.
4. Gastric Cancer
- Comparing the surgical performance of the RAG(Robot-Assisted Gastrectomy) group and the LAG
(Laparoscopic-Assisted Gastrectomy) group in gastric cancer, there was no difference in mortality rate and
complication rate. The postoperative hospital stay in RAG(Robot-Assisted Gastrectomy) group was slightly
shorter than in the LAG(Laparoscopic-Assisted Gastrectomy) group.
- Considering the robotic surgery is the early stages in gastric cancer, the precise evaluation of surgical
outcomes in clinical practice is necessary through the prospective randomized controlled study after
overcoming the learning curve.
5. Thyroid Cancer
- Robot-assisted surgery for thyroid cancer is not minimally invasive technique but remote access technique
so that it runs contrary to the view of robot-assisted surgery for other oncological disease, such as prostate
cancer, which bring less pain or recovery faster up as the main strong points. In addition, it should be
considered that new complications, brachial plexus injury, are reported even if it is rare.
- Considering very high cost for robotic thyroid surgery and lack of evidence on the surgical effectiveness, social
consensus is essential to determine if the robot-assisted surgery is appropriate for patient with thyroid cancer.
- Well designed long term follow-up prospective studies are also needed to evaluate clinical safety and
effectiveness based on sufficient quantity of evidence.



 연구정보
연구보고서
연구정보
연구보고서









 · 저작자표시
· 저작자표시 · 출처표시
· 출처표시



