□ 서 론
건강보험의 보장성 강화 노력은 지속되었지만 건강보험 보장률이 정체되고 있다. 이는 보장성 강화가 급여항목을 중심으로 이루어졌지만, 실제 비급여 의료비가 급여비에 비해 2배 정도 빠르게 증가하기 때문이다. 이는 고가의 신의료기술 신규유입과 함께 자율적인 가격제와 진료비 청구, 심사 등 관리체계 부재를 그 원인으로 설명하고 있다. 그러므로 비급여항목에 대한 적절한 의사결정은 건강보험 보장성 강화 및 국민의료비의 효율적 사용을 위해서 반드시 필요한 노력이지만 실제로 다루어지지 않았다. 2013년 보건복지부는 4대 중증질환 의료보장성 강화방안으로 선별급여를 새롭게 도입하여 비급여의 많은 부분을 급여영역으로 포함하고자 한다. 따라서 본 연구에서는 4대 중증질환 주치료목적의 처치 및 수술 비급여항목에 대한 근거평가를 통해 관련 정책결정에 활용할 수 있는 기초자료를 제공하고자 한다.
□ 연구방법
법정비급여 중 4대 중증질환(암, 심혈관계질환, 뇌혈관계질환, 희귀난치성질환)의 치료를 위해 이용되는 14개 처치 및 수술을 평가대상으로 최종 선정하였다.

14개 항목에 대해 문헌조사(임상연구, 임상가이드라인, 외국보험등재여부)와 임상전문가 자문을 통한 예비평가(Preliminary assessment)를 진행하였으며, 이 결과에 따라 신속평가(Rapid Systematic Review)가 필요한 항목인지를 결정하였다. 예비평가를 통해 임상적 문헌(임상연구 및 임상가이드라인)이 부족하고 현재 국내 사용량이 많지 않은 항목에 대해서는 신속평가(Rapid Systematic Review)를 진행하지 않았다. 즉 예비평가를 통해 신속평가를 위한 문헌의 양이 부족하거나 거의 사용되지 않은 경우 신속평가를 진행하지 않았으며, 예비평가를 통해 신속평가가 필요한 항목이라고 판단된 항목은 임상적 유용성에 대한 근거를 평가하였다(표 1). 예비평가와 신속평가를 통한 근거평가 결과에 대해서는 관련 분야 임상전문가 검토가 이루어졌으며, 필요시 검토결과를 수정․보완하는 과정을 거쳤다.
□ 연구결과
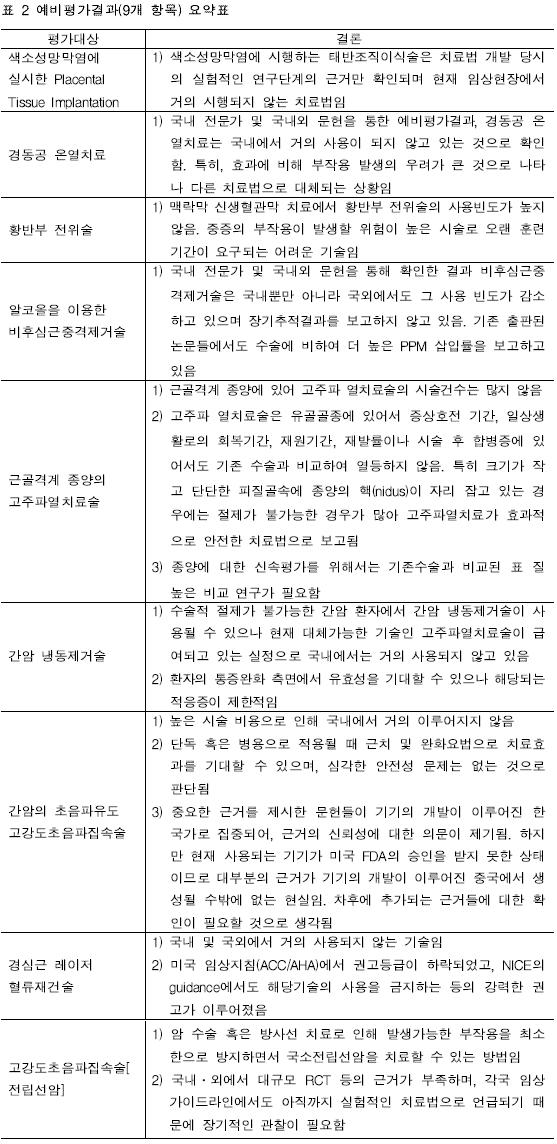
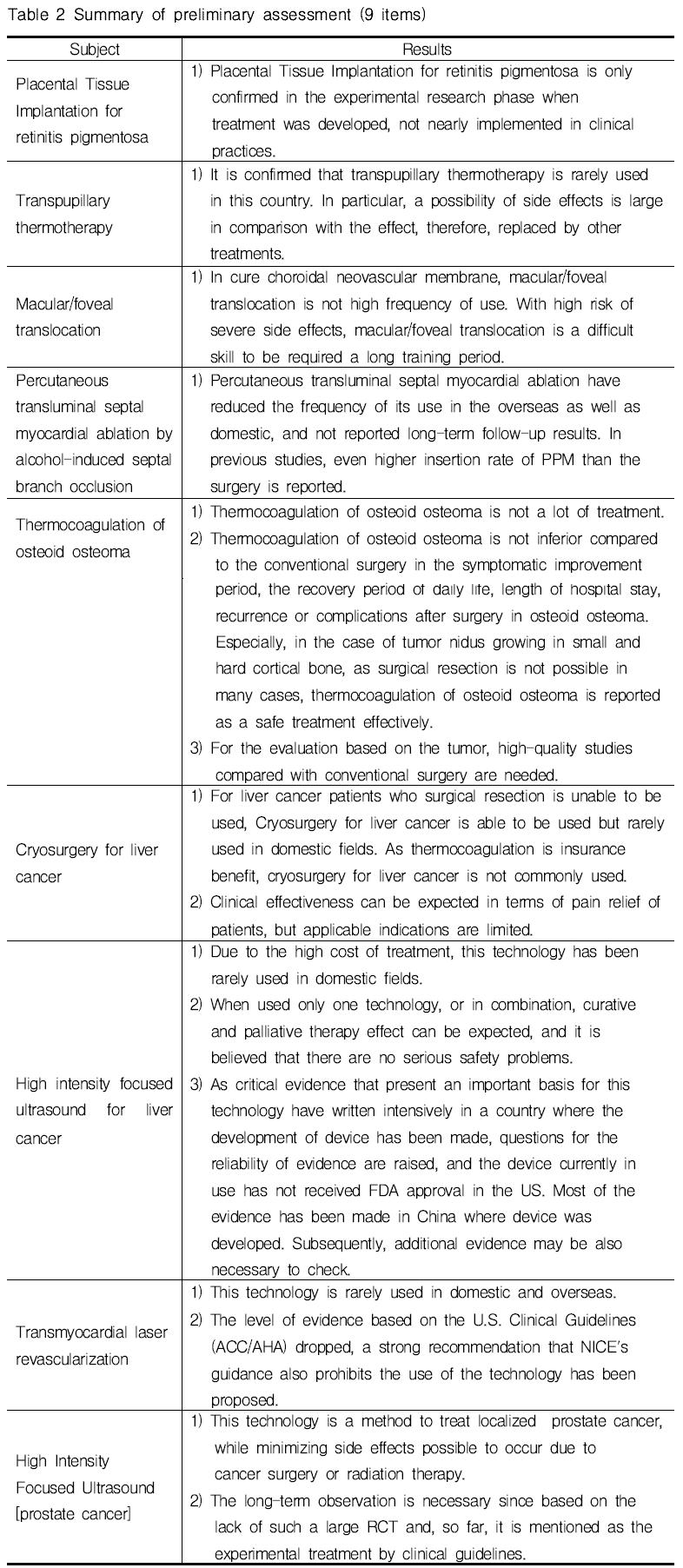
14개 항목 중 9개 항목(색소성망막염에 실시한 Placental Tissue Implantation, 경동공 온열치료, 황반부 전위술, 알코올을 이용한 비후심근중격제거술, 간암냉동제거술, 간암의 초음파유도 고강도초음파집속술, 경심근 레이저 혈류재건술, 고강도 초음파 집속술(전립선암))은 문헌평가(임상연구, 임상가이드라인, 외국의 보험여부) 및 국내 임상전문가 자문(관행수가)결과 신속평가가 필요하지 않은 것으로 파악되었다. 신속평가를 시행하지 않은 항목은 대체기술과의 상대적 효과성을 비교할 수 있는 연구가 부재하고 비교군이 없는 사례연구(case-series)만이 존재하거나, 대체기술의 발달로 인해 해당 기술의 사용이 거의 이루어지지 않은 경우들이다. 실제 9개 항목(표 2)은 급여여부결정시 검토된 근거수준에서 크게 변화하지 않은 것으로 파악되었다. 즉 비급여 결정 이후 급여전환을 위한 추가적인 근거생성이 이루어지지 않은 것으로 판단된다.
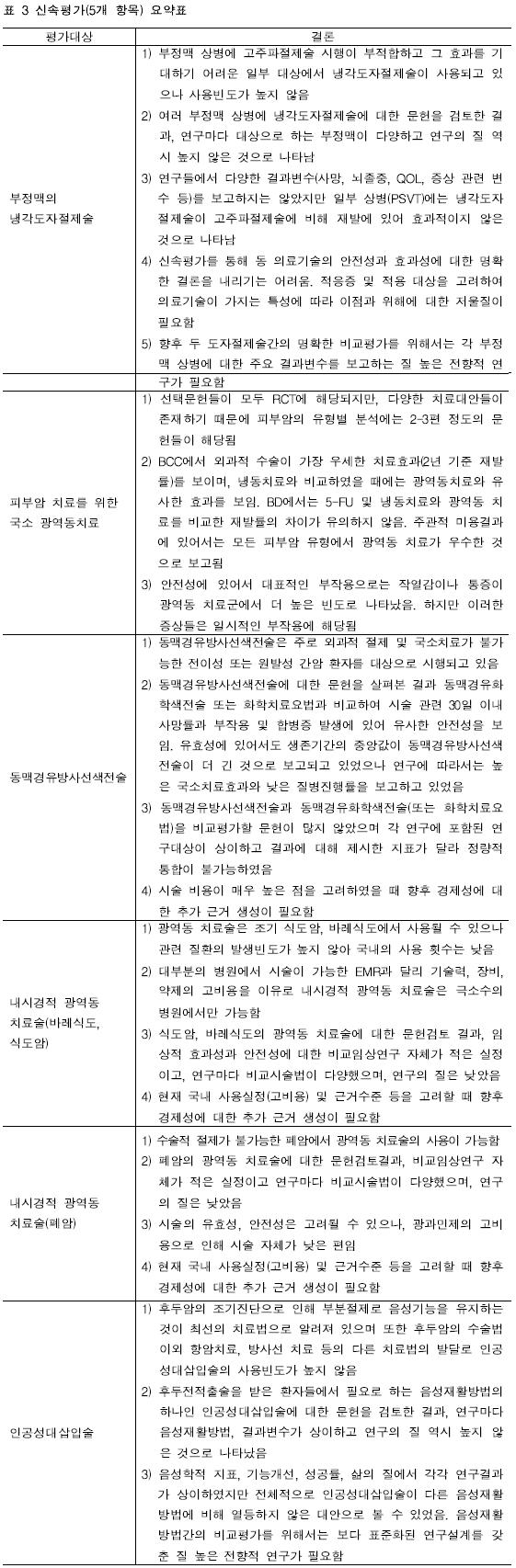
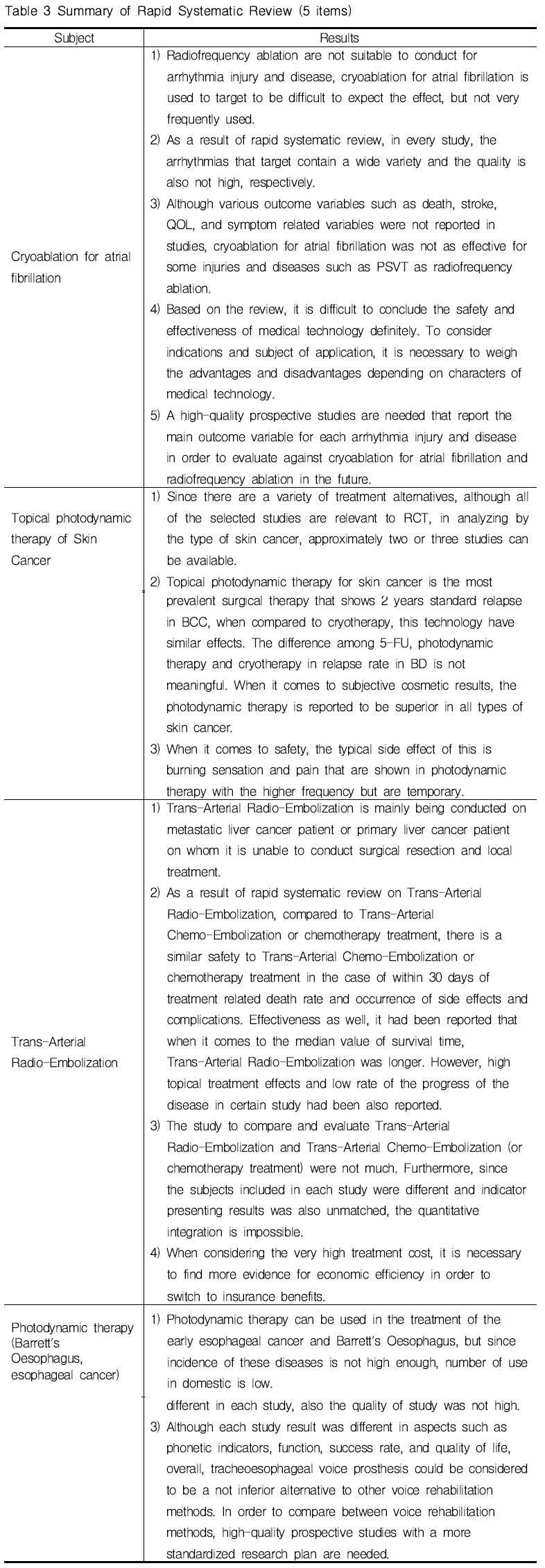
예비평가를 통해 신속평가(Rapid Systematic Review)가 필요하다고 판단한 5개 항목(부정맥의 냉각도자절제술, 피부암 치료를 위한 국소 광역동치료, 동맥경유방사선색전술, 내시경적 광역동 치료술, 인공성대삽입술)에 대한 평가결과는 <표 3>과 같이 정리할 수 있었다. 5개 항목 모두 대체가능한 처치 혹은 수술과의 비교문헌들의 질이 높지 않고 근거가 불충분(insufficient)한 수준으로 해당 항목의 임상적 유용성에 대해 결론을 내릴 수 없었다. 다만 몇몇 항목(동맥경유방사선색전술, 내시경적 광역동 치료술)의 경우에는 일부 적응증에서 효과가 다른 대안에 비해 우수하다고 확인되어 해당 영역에서 경제성에 대한 추가검토 등을 통해 급여 혹은 선별급여로의 전환을 고려할 수 있을 것으로 판단된다.
□ 결론 및 정책적 제언
지금까지 연구와 정책은 급여영역을 중심으로 이루어져왔지만 비급여 항목의 비용의 증가속도가 건강보험급여보다 2배 정도 빠르게 증가하는 비급여의 풍선효과를 고려한다면, 비급여항목에 대한 관리기전 없이는 보장성 강화 정책의 효과를 기대하기에는 한계가 있다. 이에 보건복지부는 4대 중증질환을 중심으로 선별급여를 새롭게 도입하여 이를 극복하고자 하였다.
따라서 본 연구에서는 4대 중증질환의 보장성 강화 정책을 지원하기 위해 의료기술평가관점에서 처치 및 수술항목에 대한 평가(예비평가 및 신속평가)를 시행하였다. 그 결과, 실제 이미 다른 기술로 대체되어 거의 사용되지 않는 비급여 기술들이 포함되어 있거나 임상적 유용성에 대한 근거가 불충분한 항목들이 다수 법정 비급여 항목에 포함되어 있었다. 4대 중증질환의 선별급여제도를 고려한다면, 본 연구에서 평가한 14개 법정비급여항목이 선별급여로 분류될 수 있어 본 연구결과를 관련 정책결정의 근거자료로 활용될 수 있을 것으로 기대된다. 더욱이 기존 제도에서 의료기술평가를 통한 의사결정이 이루어지지 않았던 터라 임상적 유용성에 대한 검토 없이 보험권에 도입된 법정비급여항목들이 존재할 수 있으므로 본 연구에서의 근거평가(예비평가 및 신속평가)방법을 처치 및 수술이 아닌 4대 중증질환의 다른 영역의 비급여항목에 대해서도 적용해볼 수 있을 것이다.
Evidence Assessment on Intervention and Surgery of Non-benefit Medical Care
□ Introduction
Although the efforts on the benefit extension policy of National Health Insurance (NHI) have been made around benefit medical care, non-benefit medical care fees have been actually increased rapidly twice as much as benefit medical fees.
The cause of this phenomenon can be given to new influx of high-priced new health technologies, no regulating price system, and absence of management system such as medical fee claims and reviewing in non-benefit item. Therefore, the appropriate decision for non-benefit medical care items could be essential for enhancing insurance benefit and efficient use of national health resource, but actually reviews of pay for the item have been mainly made by. In 2013, Ministry of Health and Welfare (MOHW) in Korea has introduced 'selective-benefit medical care' for benefit extension policy focusing on four severe disease (cancer, cardiovascular disease, cerebrovascular disease, and a rare disease). The purpose of this study is to provide the evidence relevant to policy through evidence assessment related to intervention and surgery of non-benefit items focusing on four severe diseases.
□ Method
14 items among 98 non-medical benefit items that were mainly used for the treatment of the four severe diseases(cancer, cardiovascular disease, cerebrovascular disease, and a rare disease) were selected as the final evaluation subjects.
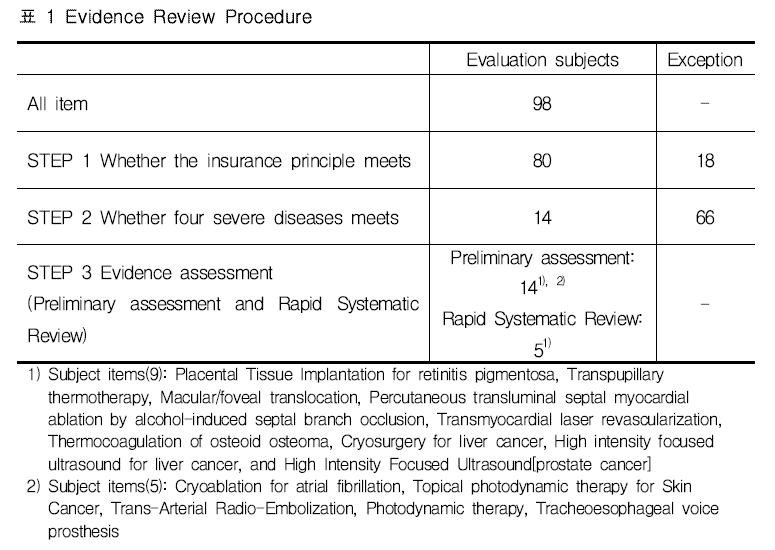
Of 14 items, a preliminary assessment including literature review(clinical research, clinical guideline, whether insurance benefit in other countries) and consultation with clinical experts was conducted. According to the results of preliminary assessment, target items of rapid systematic review was selected. Items that clinical research lacked (low evidence) and rare domestic use demand (low societal need) considered through preliminary assessment was not selected for rapid systematic review, and otherwise rapid systematic review was conducted (Table 1). Results of evidence assessment including preliminary assessment (14 items) and rapid systematic review (5 items) was looked back by clinical experts in related fields and revised if it is needed.
□ Results
As a results of preliminary assessment, 9 items (Placental tissue implantation for retinitis pigmentosa, Transpupillary thermotherapy, Macular/foveal translocation, Percutaneous transluminal septal myocardial ablation by alcohol-induced septal branch occlusion, Thermocoagulation of osteoid osteoma, Cryosurgery for liver cancer, High intensity focused ultrasound for liver cancer, Transmyocardial laser revascularization, and High Intensity Focused Ultrasound [prostate cancer]) of 14 items were confirmed that the rapid systematic review is not essential.
When it comes to the items that the rapid systematic review were not conducted, case-series that there was no comparison group on the research existed only or the technologies were rarely used due to the development of alternative technologies. In fact, 9 items (Table 2) were confirmed that evidence level was not changed significantly from the level reviewed when to determine whether insurance benefit or not. In other words, additional efforts of evidence generation about relative effectiveness comparing with alternative for switch to insurance benefit is not almost done after the decision to be uninsured.
The results of rapid systematic review on the 5 items (Cryoablation for atrial fibrillation, Topical photodynamic therapy for Skin Cancer, Trans-Arterial Radio-Embolization, Photodynamic therapy, Tracheoesophageal voice prosthesis) was summarized in Table 3.
When it comes to all 5 items, the quality of evidence comparing with alternatives is not high and is too insufficient to conclude for the relative effectiveness of all the items. Further, in the case of some items(Trans-Arterial Radio-Embolization and Photodynamic therapy), evidence for economic efficiency was checked for health insurance benefit.
□ Conclusions
The matters of concern of researches and policies have revolved around reviews on insurance benefit items until now. However, when considering the balloon effect that the speed of rising cost of the non-benefit items is much faster than that of the insured items, there is a limit of benefit extension policy without management mechanisms for non-benefit items. Therefore Ministry of Health and Welfare (MOHW) in Korea has introduced ‘selective benefit medical care’ for benefit extension focusing on four severe disease and tried to overcome it.
In this study, evidence assessment (preliminary assessment and rapid systematic review) with HTA approach was conducted for supporting benefit extension policy. As a result of reviewing in this study, in fact, the non-benefit items can be also confirmed, which are already replaced by other techniques.
Moreover, because of the part that decision was not made based on HTA results under the existing systems, there are items used without sufficient evidence. When considering the selective benefits plan of the four severe diseases that 14 items would be classified as the selective benefits. Therefore, when classifying as the selective benefits items, this study could be used as evidence of the relevant policy-making, furthermore, this study approach could be applicable to other field.



 연구정보
연구보고서
연구정보
연구보고서









 · 저작자표시
· 저작자표시 · 출처표시
· 출처표시



