□ 서 론
경동맥 협착증은 경동맥이 좁아지는 질환으로 허혈성 뇌졸중 원인의 30%를 차지하고 있으며 국내에서도 서구화된 식습관 등으로 인해 발병이 급증하고 있다. 경동맥 협착의 가장 흔한 원인은 죽상동맥경화증이며, 고혈압, 고지혈증, 당뇨병과 같은 성인병과 깊은 관련이 있다. 모든 환자에게 증상이 있는 것은 아니며 무증상의 경우 2∼3%가 뇌졸중 위험을 가지고 있는 것으로 알려져 있으며 유증상의 경우 뇌졸중 위험이 10∼17%로 알려져 있다.
경동맥 협착증을 동반한 허혈성 뇌졸중 환자에서 경동맥 내막 절제술은 재발을 막기 위한 보편적 치료로 이용되고 있으며 선택적으로는 무증상 환자에서 예방적으로 시행되기도 한다. 스텐트 삽입술은 내막절제술에 대한 고위험 환자나 병변이 머리쪽으로 높게 위치하여 수술적 접근이 불가능한 환자를 위한 치료로 개발되었다. 국내 관련 임상가이드라인(뇌졸중임상연구센터, 2011)에서는 유증상 경동맥 협착(50% 이상)을 가진 환자에서 6% 미만의 뇌졸중 발생률 또는 사망률이 예측되는 경우 스텐트 삽입술이 내막절제술의 대체치료로 사용될 수 있다고 권고(근거수준 1b, 권고수준 A)하고 있다.
따라서 본 연구에서는 경동맥 협착증에서 스텐트 삽입술이 내막절제술의 대체치료로 사용이 가능한 유증상 경동맥 협착(협착률 50% 이상)을 가진 환자를 대상으로 한국적 상황에서 두 시술의 임상적 효과성(clinical effectiveness)과 비용-효과성(cost-effectiveness)을 평가하였다. 해당 연구목적을 달성하기 위한 4개의 세부연구주제는 다음과 같다. 첫째 건강보험 청구자료를 활용하여 국내 유증상 경동맥 협착증 환자의 스텐트 삽입술과 내막절제술 시술현황 분석하였고, 둘째 유증상 경동맥 협착증 환자에서 두 시술을 비교한 무작위임상시험을 대상으로 체계적 문헌고찰을 통하여 두 시술의 임상적 효과 비교하였고, 셋째, 국내 5개 병원에서 후향적으로 수집된 의무기록을 이용 유증상 경동맥 협착증 환자에서 두 시술의 임상적 효과를 비교하였으며, 마지막으로 유증상 경동맥 협착증 환자에서 두 시술의 비용-효과를 분석하였다.
□ 유증상 경동맥 협착증 환자의 국내 의료이용 현황
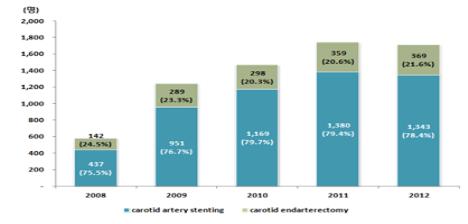
건강보험 청구자료(2008년 1월~2012년 12월)에서 경동맥 스텐트 삽입술 또는 내막절제술을 받은 환자 중 유증상 경동맥 협착증 환자 6,622명을 대상으로 현황을 분석하였다. 2008년 이후 유증상 경동맥 협착으로 인해 시술을 받은 환자는 꾸준히 증가하고 있으며, 매년 전체 시술자 중 약 80% 환자가 스텐트 삽입술을 받고 있는 것으로 나타났다(그림 3-2). 시술 대상자의 대부분은 남성이었으며 평균 연령은 스텐트 삽입술 69.95세(±8.71), 내막절제술 68.08세(±7.91)로 두 군에 차이가 없는 것으로 나타났다. 두 시술간의 치료비용과 입원일수를 비교한 결과 스텐트 삽입술의 입원당 청구비용은 7,538,590원으로 내막절제술(5,742,767원)에 비해 약 200만 원 정도 더 많았으나 입원일수는 내막절제술이 평균 14.3일로 스텐트 삽입술(13.4일)에 비해 1일 정도 길었다.
국내 유증상 경동맥 협착증 환자에서 치료비용이 높은 스텐트 삽입술의 사용빈도가 약 80%로 월등히 높은 것으로 나타났으며, 이는 미국(Goddney 등, 2010; Skerritt 등, 2012; Vogel 등, 2009)에서 내막절제술이 월등히 높은 빈도로 사용되는 것과는 반대되는 상황이다.
□ 체계적 문헌고찰을 통한 두 시술간 임상적 효과비교
기존의 체계적 문헌고찰을 활용(using existing systematic reviews)하여 유증상 경동맥 협착증 환자에서 내막절제술과 스텐트 삽입술의 임상적 효과를 비교하였다. 체계적 문헌고찰의 핵심질문은 “유증상 경동맥 협착증 환자에서 스텐트 삽입술이 경동맥 내막절제술 만큼 임상적으로 효과적인가?”이다.
본 연구의 핵심질문에 맞는 체계적 문헌고찰 4편 중 AMSTAR를 통한 질평가에서 질이 우수하다고 평가된 Bonati 등(2012)의 논문이 최종 선정되었다. Bonati 등(2012)의 연구 이후 추가로 출판된 무작위임상시험이 없어 본 연구에서는 최종 선정된 체계적 문헌고찰(Bonati 등, 2012)에 포함된 무작위임상시험 15개(18편) 중 무증상 환자를 대상으로 하거나, 유증상과 무증상을 별도로 추출할 수 없는 연구, 비비교연구, 영어문헌이 아닌 연구 등을 제외하고 최종 11개의 무작위임상시험을 대상으로 메타분석을 수행하였다.
시술 후 30일 이내 단기 임상적 효과를 비교한 결과에서는 뇌졸중, 주요뇌졸중, 사망 또는 뇌졸중, 그리고 사망, 뇌졸중 또는 심근경색의 발생위험이 내막절제술군에 비해 스텐트 삽입술군에서 통계적으로 유의하게 높은 것으로 나타났다. 심근경색의 경우에는 내막절제술에서 스텐트 삽입술에 비해 발생위험이 통계적으로 높았다. 시술 후 최종 추적관찰기간까지 주요결과를 살펴본 결과, 뇌졸중, 사망 또는 뇌졸중, 사망, 뇌졸중 또는 심근경색의 발생위험이 내막절제술에 비해 스텐트 삽입술에서 통계적으로 유의하게 높은 것으로 나타났다. 시술관련 합병증의 경우 재협착, 출혈의 경우 통계적으로 유의하지 않았으며 뇌신경마비 발생위험이 스텐트 삽입술에 비해 내막절제술에서 유의하게 높았다(표 4-8).
□ 후향적 의무기록조사를 통한 두 시술간 임상적 효과비교
국내 경동맥 협착증 환자에서 내막절제술과 스텐트 삽입술간의 임상적 효과를 비교하기 위해 5개 의료기관(인하대병원, 삼성서울병원, 서울아산병원, 전남대병원, 신촌세브란스 병원)에서 2008년부터 2011년까지 협착률 50% 이상의 유증상 경동맥 협착증으로 내막절제술 또는 스텐트 삽입술을 받은 환자 677명(내막절제술 331명, 스텐트 삽입술 346명)을 분석하였다.
시술대상자 677명의 평균연령은 68세였으며, 남성이 80% 이상을 차지하였다. 또한 유증상 경동맥 협착증의 협착률 70% 이상의 비율이 스텐트 삽입술의 경우 90.2%, 내막절제술 75.5%로 스텐트 삽입술을 받았던 환자에서 협착률이 유의하게 높았다(p<0.001). 스텐트 삽입술을 받은 환자의 96.8%에서 EPD가 사용되었다(표 5-5).
시술 후 30일 이내 사망, 뇌졸중, 심근경색의 발생률을 비교한 결과 스텐트 삽입술에서의 뇌졸중 발생이 통계적으로 유의하게 높았다(CAS 4.99%, CEA 1.89%, p<0.026) (표 5-6). 시술 후 2년까지 추적 관찰한 경우에서는 사망, 뇌졸중, 심근경색 발생 모두 두 시술간 통계적으로 유의한 차이를 보이지 않았다. 2차 결과지표로 살펴본 뇌신경마비, 수술 중 합병증, 재시술 여부에서는 장․단기 모두에서 뇌신경마비의 발생이 내막절제술에서 유의하게 높은 결과를 보였다(표 5-7; 표 5-8).
협착률과 연령군에 따른 하위군 분석을 시행한 결과, 협착률 70% 이상의 고위험군(562명)에서 시술 후 2년 이내 중증 뇌졸중의 발생률이 스텐트 삽입술군(312명)이 내막절제술군(250명)에 비해 통계적으로 유의하게 높았다(CAS 4.99%, CEA 1.84%, p<0.024). 2차 결과지표 중 뇌신경마비는 협착률 70% 이상군에서 내막절제술군에서 통계적으로 유의하게 높게 발생하는 것으로 나타났다(표 5-13). 연령에 따른 하위군 분석에서는 70세 미만군에서는 장․단기 사망, 뇌졸중, 심근경색의 발생이 두 군간에 차이가 없었다. 70세 이상군에서는 시술 후 30일 이내 뇌졸중의 발생률이 스텐트 삽입술에서 통계적으로 유의하게 높았다(p<0.044). 2차 결과지표 중 뇌신경마비는 두 연령군 모두 에서 내막절제술에서 유의하게 높게 발생하였다(표 5-15; 표 5-16; 표 5-17).
본 후향적 연구결과는 체계적 문헌고찰을 통하여 검토된 기존의 무작위임상연구들과 비교 할 때 사망, 뇌졸중, 그리고 심근경색 등의 합병증 발생이 경동맥 스텐트 삽입술에서 높았다는 결과는 유사하였으나 절대적인 발생률은 낮았다. 국내에서 이루어진 후향적 연구 2편(함형용 등, 2011; 윤우성 등, 2011)과의 비교에서도 본 연구에서 보고한 뇌졸중, 심근경색, 사망의 발생빈도가 더 낮았다. 함형용 등(2011)은 1999~2010년 동안 후향적 조사로 시술 30일 기준 뇌졸중, 사망 발생을 확인한 결과, 스텐트 삽입술군에서의 발생률이 내막절제술군에 비해 높았으나(내막절제술 1.79%, 스텐트 삽입술 6.06%), 두 군간의 통계적으로 유의한 차이를 보이지 않았다. 윤우성 등(2011)의 연구에서도 비슷한 결과를 보였다(시술 30일 기준 뇌졸중, 내막절제술 1.45%, 스텐트 삽입술 9.52%). 이는 본연구에서 비교효과연구라는 연구목적을 달성하기 위해 연구대상 배제 포함 기준을 매우 엄격하게 설정하였기 때문일 수도 있을 것이다.
□ 경동맥 협착증 관련 건강상태의 삶의 질 조사
건강관련 삶의 질을 고려한 경제성 평가 수행을 위해 본 연구에서는 경동맥 협착증과 관련된 건강상태별 효용값(utility index)을 조사하였다. 건강상태는 경동맥 협착증으로 내막절제술 혹은 스텐트 삽입술 후 뇌졸중과 심근경색과 같은 주요 합병증은 없는 상태, 심근경색이 발생한 상태, 경증 뇌졸중 혹은 중증 뇌졸중 상태로 구분하였다. 시술 후 주요 합병증이 발생하지 않은 상태는 가상의 시나리오를 제공하고 일반인 400명을 대상으로 시간교환법(Time Trade Off, TTO)과 EQ-5D-3L 도구를 활용하여 효용값을 조사하였다. 심근경색은 제5기 국민건강영양조사(2012) 자료에서 중증도별 뇌졸중은 분당서울대병원 뇌졸중 레지스트리(환자 465명)에서 각각 효용값을 추정하였다.
설문조사 결과 경동맥 협착증으로 내막절제술 혹은 스텐트 삽입술 후 주요 합병증이 발생하지 않은 건강상태의 효용값은 0.79(±0.10)로 평가되었다. 하지만 재협착으로 인해 재시술을 받은 이후의 건강상태에 대해서는 0.61(±0.13)로 낮게 평가하였다. 심근경색의 효용값은 0.77(±0.05), 경증 뇌졸중은 0.79(±0.06), 중증 뇌졸중 0.41(±0.48)로 나타났다(표 6-8). 결론적으로 경동맥 협착증 환자들에서 가장 삶의 질이 낮을 것이라 평가된 것은 중증 뇌졸중 이었고 재협착으로 인한 재시술, 심근 경색, 경증 뇌졸중의 순으로 낮게 평가되었다. 시술 후 주요 부작용이 없는 상태와 경증 뇌졸중이 있는 상태는 유사한 삶의 질로 평가되었다.
□ 국내 경동맥 협착증 환자에서 두 시술간 비용-효용분석
본 연구에서는 보건의료체계관점에서 유증상 경동맥 협착증(협착률 50% 이상) 환자를 대상으로 스텐트 삽입술과 내막절제술의 비용-효용분석을 수행하였다. 비용-효용분석은 15년 분석기간 동안 비용과 질보정수명(Quality adjusted Life Years, QALYs)을 추정하는 마콥모형으로 시행하였다.
전이확률 및 효과는 앞서 언급한 국내 유증상 경동맥 협착증 환자 677명을 대상으로 한 후향적 의무기록조사자료를 이용하여 추정하였다. 비용은 보건의료체계관점에서 시술관련 비용으로 시술 및 처치, 검사, 마취, 약제비, 입원비, 간병비를 포함하였고, 합병증으로 인한 비용으로 뇌졸중, 심근경색, 시술로 인한 뇌신경마비 치료비용을 포함하였다. 교통비용은 두 군 간의 차이가 없어서 별도로 산출하지 않았으며, 대상 환자의 평균 연령이 68세 이상으로 진료로 인한 추가적인 근로시간의 손실이 발생하지 않을 것으로 가정하고 시간비용을 포함하지 않았다. 시술비용과 합병증으로 인한 치료비용의 경우 비급여 비용까지 모두 포함하였으며 할인율 5%를 적용하였다. 시술 비용은 내막절제술 367만원, 스텐트 삽입술이 603만원으로 추정되어 스텐트 삽입술의 시술 비용이 약 240만원 더 많았다. 시술로 인해 발생한 주요 합병증 치료비용에서 시술 후 30일까지 주요합병증이 없는 건강상태는 내막절제술이 152만원으로 스텐트 삽입술 118만원보다 약 40만원 더 많았으며 이는 입원일수의 차이로 인한 것으로 판단된다. 각 시술 이후 발생한 심근경색, 뇌졸중의 경우는 시술별로 두 질환의 치료비용이 다르지 않을 것으로 보고 각 질환의 치료비용을 두 시술 군에 동일하게 적용하였다.
비용-효용분석을 시행한 결과 협착률 50% 이상의 유증상 경동맥 협착증 환자가 내막절제술을 받을 경우 질보정수명(QALYs)이 6.71년으로 스텐트 삽입술(6.49년)을 받을 경우보다 약 0.22년 더 긴 것으로 분석되었다. 또한 내막절제술의 비용은 15년간 1인당 약 798만원, 스텐트 삽입술은 약 967만원이 발생하는 것으로 추정되었다. 즉 유증상 경동맥 협착증 환자(협착률 50% 이상)에서 경동맥 내막절제술이 스텐트 삽입술에 비해 비용은 적게 들고, 효과는 다소 좋은 시술로 분석되었다(표 7-22). 또한 협착률(70% 기준)에 따른 하위군 분석결과에서는 협착률 70% 이상의 환자군에서의 분석결과는 기본분석과 유사하였으며, 협착률 70% 미만의 환자군에서는 스텐트 삽입술(약 652만원)이 내막절제술(1,184만원)에 비해 비용도 저렴하고 질보정수명(내막절제술: 6.01 QALYs, 스텐트 삽입술: 7.15 QALYs)이 더 긴 것으로 분석되었다. 연령군별 하위군 분석에서는 70세 이상 환자군에서는 기본분석과 유사한 결과가 나타났으며, 70세 미만 환자군에서 내막절제술 대비 스텐트 삽입술의 소요비용이 다소 낮고(내막절제술 687만원, 스텐트 삽입술 642만원), 효과는 우수한 것으로 분석되었다(내막절제술 6.90 QALYs, 스텐트 삽입술 7.17 QALYs)(표 7-30).
국내외 진료지침에서 협착률 50% 이상 유증상 경동맥 협착증에서 스텐트 삽입술이 내막절제술의 대체치료가 될 수 있다고 권고하고 있으나, 국외 유증상 경동맥 협착증 환자에서 스텐트 삽입술과 내막절제술을 비교한 다수의 경제성 평가에서 스텐트 삽입술은 비용-효과적이지 않거나 오히려 비용이 높고 효과는 낮은 것으로 나타났다. 국내의 현황을 반영한 본 연구의 경제성 평가 역시 일관된 결과를 보였다.
□ 결론 및 정책적 제언
국내에서도 경동맥 협착증의 발생빈도가 증가하고 있다. 이러한 경동맥 협착증 환자 중 유증상 경동맥 협착증(협착률 50%) 환자를 본 연구의 대상으로 선정하였다. 체계적 문헌고찰과 후향적 의무기록조사를 통해 유증상 경동맥 협착환자에서 내막절제술과 스텐트 삽입술 후 사망, 뇌졸중, 심근경색, 시술과 관련된 합병증의 발생빈도를 비교하였다. 그 결과 내막절제술에서 사망, 뇌졸중의 발생빈도는 낮았고 시술과 관련된 합병증의 발생빈도는 더 높았다. 임상적 효과결과에 근거하여 두 시술의 비용-효용분석을 시행한 결과 내막절제술과 스텐트 삽입술의 효과차이는 크지 않은 반면 내막절제술의 비용이 상대적으로 낮아 현재로서는 경제적인 치료법이었다. 이러한 결과를 일반화하기 위해서는 국내에서도 대규모 전향적, 다기관, 무작위 배정 임상연구가 시행되어야 할 것이며 이러한 비교효과연구(comparative effectiveness research, CER)를 바탕으로 경동맥 내막절제술과 스텐트 삽입술의 적절한 사용에 대한 근거를 제시할 수 있을 것으로 기대된다.
주요어: 경동맥 협착증, 내막절제술, 스텐트 삽입술, 경제성 평가
□ Background
Carotid artery stenosis is a narrowing or constriction of the inner surface of the carotid artery and is serious because it can cause a stroke. 30% of the cause of stroke is from this disease and occurrence of this disease is rapidly increasing in Korea because of the lifestyle changes. The narrowing of the carotid arteries is most commonly related to atherosclerosis, and it is closely related with adult diseases, such as hypertension, hyperlipidemia, and diabetes. Not all patients have symptoms; carotid artery disease may be asymptomatic or symptomatic. It is considered that 2–3% of asymptomatic carotid stenosis patients have the risk of stroke, and 10–17% of symptomatic patients have the risk of stroke.
Carotid steonsis is conventionally treated by carotid endarterectomy (CEA) as a preventive treatment of stroke, and patients with and without neurological symptoms are selectively treated with this treatment method. Carotid-artery stenting (CAS) was developed as an option for patients who are high risk for CEA or patients who has high risk because of carotid lesions located at or above the level of the second cervical vertebra. Clinical guideline in Korea recommends (Level of Evidence 1b, Classification of Recommendation A) that CAS indicated as an alternative to CEA for symptomatic patients who have more than 50% stenosis and the anticipated rate of stroke or mortality is less than 6% (Clinical Research Center For Stroke, 2011).
Therefore, this study evaluated the clinical effectiveness and cost-effectiveness in the target patients with symptomatic carotid artery stenosis (more than 50% stenosis) who can undergo CAS as an alternative to CEA for carotid artery stenosis. The four detailed topics to achieve the object of this study are the following: first, the utilization trends (2008-2012) of the treatments (CEA and CAS) in patients with symptomatic carotid artery stenosis in Korea by using national health insurance claims database provided HIRA; second, the comparative effectiveness of the CEA and CAS based on systematic reviews in patients with symptomatic carotid artery stenosis; third, the comparative effectiveness of the CEA and CAS based on retrospective chart review of patients with symptomatic carotid artery stenosis (>50%) collected from five hospitals in Korea (2008-2011); fourth, the cost-utility analysis of CEA versus CAS in patients with symptomatic carotid artery stenosis.
□ Utilization Trends of Patients with Symptomatic Carotid Artery Stenosis in Korea
The utilization trend was analyzed from the database of Health Insurance Review and Assessment Service (HIRA; Seoul, Korea) between 1 January 2008 and 31 December 2011. The number of patients with symptomatic carotid artery stenosis among the patients who received CAS or CEA were 6,622. The number of patients who received a carotid intervention is increasing since 2008, and the result appeared that about 80% among all symptomatic carotid stenosis patients received CAS annually (Figure 1).
Most of the patients undergoing the carotid intervention (CEA or CAS) were male and the average age of patients who received CAS was 69.95 (±8.71) years while that of patients who received CEA was 68.08 (±7.91) years — there was not much difference between the groups.
As a result of the comparison treatment cost and the length of hospital stay for both procedures, the treatment cost per hospitalization for CAS KRW 7,538,590, which was more expensive than CEA (KRW 5,742,767), but length of hospital stay for CEA was 14.3 days in average, which was slightly longer than CAS (13.4 days).
□ A Systematic Review: Comparative Effectiveness between CAS and CEA in Patients with symptomatic Carotid Stenosis
By using existing systematic review, clinical effectiveness of CEA and CAS in patients with symptomatic carotid artery stenosis was compared. The research question in this systematic review was: “Dose CAS has significantly different risk of peri-procedural stroke or death compared with CEA in patients with symptomatic carotid artery stenosis?”
Among the four systematic reviews in accordance with the key question of this study, an article published by Bonati et al. (2012) was finally selected because it was evaluated as a good methodological quality through AMSTAR (assessment of multiple systematic reviews). There was no other randomized control trial (RCT) published after the study by Bonati et al. (2012). We excluded obviously irrelevant studies (excluding the studies in patients with asymptomatic carotid stenosis, a study that cannot extract symptomatic and asymptomatic patients separately, non-comparative study, and non-English study) from 15 RCT included in the systematic review (Bonati et al., 2012). Therefore 11 RCTs involving 5,621 patients with available outcome data that fulfilled the inclusion criteria was included. Main results of meta-analysis were shown <Table 1>.
|
|
CAS |
CEA |
Meta-analysis result
(Reference group: CEA) |
|
RR |
95% lower |
95% upper |
|
Peri-procedure outcome (within 30 days after treatment) |
|
Death |
26/1,943 |
15/1,938 |
1.72 |
0.90 |
3.30 |
|
Any stroke |
206/2,621 |
120/2,598 |
1.72 |
1.28 |
2.30 |
|
Major stroke1) |
83/2,611 |
57/2,588 |
1.43 |
1.03 |
2.00 |
|
Myocardial infarction (MI) |
11/2,555 |
25/2,539 |
0.46 |
0.23 |
0.93 |
|
Death or any stroke |
227/2,669 |
132/2,661 |
1.75 |
1.31 |
2.33 |
|
Death or any stroke or MI |
144/1,727 |
100/1,715 |
1.43 |
1.12 |
1.83 |
|
Post-procedure outcome (until the end of follow-up) |
|
Death |
93/1,793 |
75/1,784 |
1.25 |
0.86 |
1.81 |
|
Any stroke |
207/2,461 |
142/2,437 |
1.44 |
1.1 |
1.89 |
|
Major stroke1) |
68/1,629 |
50/1,627 |
1.3 |
0.9 |
1.88 |
|
Death or any stroke |
184/2,200 |
128/2,178 |
1.4 |
1.02 |
1.93 |
|
Death or any stroke or MI |
152/1,624 |
107/1,610 |
1.42 |
1.04 |
1.94 |
|
Peri-procedure complication |
|
Restenosis |
14/614 |
2/600 |
3.71 |
0.31 |
44.48 |
|
Hemorrhage |
29/1,853 |
42/1,828 |
0.75 |
0.19 |
2.91 |
|
Cranial nerve palsy |
7/1,853 |
103/1,828 |
0.1 |
0.05 |
0.2 |
|
1) Major stroke: Major, fatal, or disabling stroke |
The risk of stroke of any severity, occurring between randomization and 30 days following the procedure was significantly higher in CAS group compared with the CEA group (RR: 1.72, 95% CI: 1.28-2.30). There was also significant difference in the major stroke (major, fatal or disabling stroke), and two combined outcome measures of ‘death or any stroke’, and ‘death or any stroke or myocardial infarction (MI)’ between CEA and CAS (Table 1). The risk of myocardial infarction (MI) up to 30 days after treatment was lower in patients assigned to CAS than in CEA groups (RR: 0.46, 95% CI: 0.23-0.93). There was a non-significant increase in all-cause mortality up to 30 days after treatment among patients randomized to CAS compared with those assigned CEA (RR: 1.72, 95% CI: 0.90-3.30). According to the major results during follow-up period after the treatment, the risk of any stroke, ‘death or any stroke’, and ‘death or any stroke or myocardial infarction (MI)’ was significantly higher in CAS compared with CEA. In case of the other complications related with the treatment, rates of cranial nerve palsy were significantly reduced among patients treated CAS compared with CEA (RR: 0.1, 95% CI: 0.05-0.2). The overall comparison did not showed higher restenosis or hemorrhage rates among patients assigned CAS compared with CEA patients.
□ A Multi-center, Retrospective Chart Review: Comparative Effectiveness between CAS and CEA in Korean Patients with Symptomatic Carotid Stenosis
In this study, peri-procedure and post-procedure outcome of CAS was compared with those of CEA in patient with carotid artery stenosis in Korea. Between January 2008 and December 2011, 677 patients (CEA patients=331, CAS patients=346) with symptomatic carotid artery stenosis (≥50%) who underwent carotid intervention were enrolled in this study at five hospitals (Inha University Hospital, Samsung Medical Center, Asan Medical Center, Chonnam National University Hospital, and Severance Hospital).
Patient demographic and clinical data are shown in <Table 2>. The average age of the total patients was 68.3 (range: 24-92 years), and there were 570 males (84.2%) and 107 female (15.8%). There was no difference in age and gender between two groups. The mean follow-up duration was 499.9 days. The ratio of symptomatic carotid artery stenosis with more than 70% of stenosis was 90.2% in CAS group and 75.5% in CEA group - the degree of stenosis in the CAS group was slightly higher more than CEA. 96.8% of 346 patients underwent CAS by Embolic Protection Devices (EPDs).
|
|
Total
(N=677) |
CAS
(N=346) |
CEA
(N=331) |
|
n |
(%) |
n |
(%) |
n |
(%) |
|
Age |
|
|
|
|
|
|
|
|
Mean ± SD |
68.3 |
±8.3 |
68.5 |
±8.6 |
68.2 |
±7.8 |
|
|
[min, max] |
[24 |
92] |
[24 |
92] |
[42 |
86] |
|
|
Younger than 70 yrs |
340 |
(50.2) |
170 |
(49.1) |
170 |
(51.4) |
|
|
70 yrs or older |
337 |
(49.8) |
176 |
(50.9) |
161 |
(48.6) |
|
Gender |
|
|
|
|
|
|
|
|
Male |
570 |
(84.2) |
295 |
(85.3) |
275 |
(83.1) |
|
|
Female |
107 |
(15.8) |
51 |
(14.7) |
56 |
(16.9) |
|
Follow-up period |
|
|
|
|
|
|
|
|
No. of patient |
653 |
|
337 |
|
316 |
|
|
|
Mean ± SD |
499.9 |
±246.8 |
518.4 |
±237.0 |
480.1 |
±255.8 |
|
Degree of stenosis |
|
|
|
|
|
|
|
|
< 70% |
115 |
(17.0) |
34 |
(9.8) |
81 |
(24.5) |
|
|
≥ 70% |
562 |
(83.0) |
312 |
(90.2) |
250 |
(75.5) |
|
CAS with EPD |
|
|
|
|
|
|
|
|
Yes |
|
|
335 |
(96.8) |
- |
|
|
|
No |
|
|
11 |
(3.2) |
- |
|
|
|
CAS
(N=346) |
CEA
(N=331) |
p-value2) |
|
n |
rate(%)1) |
n |
rate(%)1) |
|
Peri-procedure outcome(within 30 days after treatment) |
|
|
Death |
2 |
(0.59) |
1 |
(0.31) |
1.000† |
|
|
Stroke |
17 |
(4.99) |
6 |
(1.89) |
0.026 |
|
|
Major |
7 |
(2.06) |
1 |
(0.30) |
0.069† |
|
|
Minor |
10 |
(2.94) |
5 |
(1.59) |
0.256 |
|
|
MI |
1 |
(0.30) |
0 |
(0.00) |
1.000† |
|
Post-procedure outcome(up to 2 years after treatment) |
|
|
Death |
5 |
(1.57) |
1 |
(0.31) |
0.217† |
|
|
Stroke |
24 |
(7.27) |
14 |
(5.05) |
0.126 |
|
|
Major |
14 |
(4.46) |
6 |
(2.40) |
0.086 |
|
|
Minor |
11 |
(3.25) |
9 |
(3.00) |
0.743 |
|
1) Kaplan-Meier method
2) Chi-square test, †: Fisher's exact test |
Among peri-procedure outcomes, 30-day stroke rate was inferior in CAS group to CEA group, and it was statistically significant (4.99% vs. 1.89%, p=0.026, chi-test). There was no significant difference between CAS and CEA for death and MI within 30 days after treatment. As a result of the analysis in the whole period (up to 2 years) after treatment, the incidence rate of death, stroke, and myocardial infarction in CAS group was higher than the CEA group, but it was not a statistically significant difference (Table 3). Peri-operative complications (infection or hemorrhage) was less common with CAS than CEA (2 patients in CAS, 4 patients in CEA), and revascularization was done in 1 patient of CAS and 1 patients of CEA group during the follow-up. Rates of cranial nerve palsy were significantly reduced among patients treated CAS compared with CEA groups (p-value< 0.001, chi-test).
We also performed subgroup analysis by degree of stenosis and age. First, as a result of the subgroup analysis based on 70% of stenosis, the rate of death, stroke, and myocardial infarction was higher in CAS group (312 patients) even in the high risk group with > 70% carotid stenosis (562 patients), and rate of major stroke was statistically inferior in CAS group to CEA group. For the patient group with less than 70% of stenosis (115 patients), 30-day stroke rate was higher in CAS (34 patients), but 2-years stroke rate was higher in CEA (81 patients), and the difference was not statistically significant. The rate of complications, the secondary outcomes, was higher CEA group than CAS in more and less than 70% stenosis group, and only the cranial nerve palsy showed statistically significant difference in more than 70% stenosis group.
Second, as a result of age subgroups analysis (younger than 70 years, 340 patients, 70 years or older, 337 patients), in 70 years or older groups, the rate of death, stroke, and myocardial infarction was higher in CAS group, but it was not statistically significant. In CAS group, younger than 70 years old (340 patients), the rate of major and minor stroke was higher, but the death rate was higher in CEA group; the result was not statistically significant.
|
F/U
Period |
Result |
Systematic Review |
Retrospective Chart Review |
|
CAS |
CEA |
CAS
(n=346) |
CEA
(n=331) |
|
N |
event |
% |
N |
event |
% |
event |
% |
event |
% |
|
Short term
F/U
(within 30 days) |
Death |
1,943 |
26 |
1.34 |
1,938 |
15 |
0.77 |
2 |
0.58 |
1 |
0.30 |
|
Stroke |
2,621 |
206 |
7.86 |
2,598 |
120 |
4.62 |
17 |
4.91 |
6 |
1.81 |
|
Major |
2,611 |
83 |
3.18 |
2,588 |
57 |
2.20 |
7 |
2.02 |
1 |
0.30 |
|
Minor |
|
|
|
|
|
|
10 |
2.89 |
5 |
1.51 |
|
MI |
2,555 |
11 |
0.43 |
2,539 |
25 |
0.98 |
1 |
0.29 |
0 |
0.00 |
|
peri-operative infection |
|
|
|
|
|
|
2 |
0.58 |
3 |
0.91 |
|
Cranial nerve palsy |
|
|
|
|
|
|
0 |
0.00 |
12 |
3.63 |
|
Long term
F/U
(From 30 days) |
Deaths |
1,545 |
142 |
9.19 |
1,519 |
139 |
9.15 |
3 |
0.87 |
0 |
0.00 |
|
Strokes |
1,502 |
33 |
2.20 |
1,475 |
36 |
2.44 |
8 |
2.31 |
9 |
2.72 |
|
Major |
615 |
14 |
2.28 |
607 |
10 |
1.65 |
7 |
2.02 |
5 |
1.51 |
|
Minor |
|
|
|
|
|
|
1 |
0.29 |
4 |
1.21 |
|
Revascularization: |
|
|
3.00 |
|
|
1.00 |
1 |
0.29 |
4 |
1.21 |
|
Retrospective studies |
|
CREST |
|
|
4.00 |
|
|
6.10 |
□ Quality of Life in the Health States related with Carotid Artery Intervention
For cost utility analysis, the utility index for health states related with carotid artery intervention was surveyed by face-to-face interview. Health states was classified in accordance with the major health states in Markov model for cost-utility analysis: no major adverse events (stroke or myocardial infarction) after CEA or CAS, myocardial infarction and stroke (minor or major stroke).
The utility index without major adverse events after treatment was surveyed by using the time trade off (TTO) and EQ-5D-3L against 400 general populations after providing a virtual scenario which is a comprehensive general description of health status of the carotid artery stenosis patient. The 5th Korea National Health and Nutrition Examination Survey (KNHNES) in 2012 data were used for the utility of myocardial infarction, and 465 patients in the stroke registry of Seoul National University Bundang hospital were analyzed for the utility index of stroke per severity.
|
Health states |
Mean |
SD |
Source of data (Instrument) |
|
No major adverse events |
|
|
|
|
After initial treatment |
0.79 |
±0.10 |
Survey (TTO) |
|
After revascularization |
0.61 |
±0.13 |
|
Myocardial infarction |
0.77 |
±0.05 |
Korea National Health and Nutrition Examination Survey (EQ-5D-3L) |
|
Minor stroke |
0.79 |
±0.06 |
Patient registry (EQ-5D-3L) |
|
Major stroke |
0.41 |
±0.48 |
As a result of TTO survey, the utility index of health states without major adverse events after CEA or CAS was 0.79 (±0.10). However, utility index of health states without major adverse event after the revascularization due to restenosis was lower, 0.61 (±0.13. The utility index of major adverse events by health states was as follow: the utility index was 0.77 (±0.05) for myocardial infarction, 0.79 (±0.06) for minor stroke and 0.41 (±0.48) for major stroke. Consequentially, utility index of health states without major adverse events after treatment was similar with minor stroke after treatment, and followed by myocardial infarction, major stroke in an order. In case of revascularization due to restenosis, respondents of TTO survey evaluated that the lower utility index due to the high risk of stroke and myocardial infarction compared with the initial treatment.
□ Cost-utility analysis of CAS as compared to CEA for patients with symptomatic carotid artery stenosis in Korea
The cost-utility analysis of CAS versus CEA was conducted for the patients with symptomatic carotid artery stenosis (≥50% stenosis) from Korean healthcare system perspectives. We used the Markov model to compare the expected costs and quality-adjusted life years (QALYs) during the 15 years of time horizon period. The health status was comprised of five states such as no major adverse events (NMAEs), myocardial infarction, major stroke, minor stroke, and death. The cycle length was 1 year. The incremental cost per the additional QALY gained of CAS compared to CEA was calculated. All future costs, and QALYs were discounted at 5% per year, consistent with current guidelines.
Transition probability and clinical outcomes were estimated based on the retrospective cohort study with a medical chart review for 677 subjects with symptomatic carotid artery stenosis in Korea. We applied the utility index of Markov health states from the survey using TTO or EQ-5D.
The costs were categorized into procedural costs and post-procedural costs related to complication. The procedural costs including the index procedure, diagnostic procedures / laboratory tests, anesthesia, and drug costs were calculated based on resource use and unit cost for each component. Also, the post-procedural costs for treatment of stroke, myocardial infarction, and cranial nerve palsy were estimated using the claims data by HIRA. Because physician visits were not significant difference between two groups, and the average age of the subjects was over aged 68 years, transportation costs and patient time costs were not considered in this study. As a result, the procedural costs per event were about KRW 2,360,000 higher for CAS (KRW 3,670,000 for CEA versus KRW 6,030,000 for CAS). Within 30-days, initial hospitalization costs for patients with NMAEs were about KRW 340,000 higher for CEA, which showed longer length of stays than CAS (KRW 1,520,000 for CEA versus KRW 1,180,000 for CAS). The post-procedural costs for treatment of stroke, and myocardial infarction was applied equally to both CEA and CEA.
For symptomatic patients with carotid artery stenosis over 50%, the cost-utility analysis demonstrated that over a 15-year time horizon CEA was associated with a 0.22 QALY gained (6.49 QALYs for CAS versus 6.71 QALYs for CEA) and net cost savings of about KRW 1,690,000 (KRW 7,980,000 for CAS versus KRW 7,980,000 for CEA). In other words, the base case analysis showed that CEA for patients with symptomatic stenosis had a slightly better benefit than CAS, with lower costs.
Subgroup analysis was performed for degree of stenosis (70%), age (70 years old) and physicians with adequate training. The results for subjects with ≥70% stenosis were similar to the base-case; For subjects with <70% stenosis, CAS (about KRW 6,520,000) was less expensive than CEA (KRW 11,840,000), and had 1.05 longer QALYs (7.15 QALYs for CAS versus 6.01 QALYs for CEA). Also, CAS for the patients younger than 70 years old was associated with the higher costs of KRW 450,000, and the 0.27 QALYs increased as compared with CEA. Meanwhile, the analyses for the patients over aged 70, and those treated by physicians with adequate training were consistent with the base case analysis. Subgroup analysis showed that CAS became the cost-effectiveness alternative for the patients under the age of 70, and <70% stenosis.
Recently, clinical practice guideline in Korea and foreign countries recommends that the CAS can be the alternative treatment for the CEA in symptomatic patients with ≥ 50% carotid artery stenosis. But previous economic evaluation studies assessed in foreign countries reported that CAS was not cost-effectiveness or it was dominated by CEA for symptomatic patients with both higher costs and lower effectiveness (Table 6). This study assessed based on the domestic data also showed a consistent result.
|
|
Study population & Comparator |
Methods and Results |
Data Source |
|
Janssen et al.
(2008) |
•Symptomatic with ≥ 70% stenosis
•CAS vs. CEA |
•Cost-Utility analysis/Time horizon: 10 years
•CEA dominant |
ECST,
Cochrane SR |
|
Young et al.
(2010) |
•Symptomatic over aged 70
•CAS vs. CEA |
•Cost-Utility analysis/Time horizon: Lifetime
•CEA dominant. |
CREST, SAPPHIRE, EVA-3S, SR |
|
Mahoney et al.
(2011) |
•Symptomatic in surgical high risk group
•CAS with EPD vs. CEA |
•Cost-Utility analysis/Time horizon: Lifetime
•ICER of CAS compared to CEA=$204,229: CAS, no cost-effectiveness
(ICER=$6,555 in asymptomatic stenosis: CAS, cost-effectiveness) |
SAPPHIRE |
|
Vilain et al.
(2012) |
•Symptomatic and asymptomatic
•CAS vs. CEA |
•Cost-Utility analysis/Time horizon: 10 years
•CAS with higher costs of $524 and lower QALYs of 0.008: CAS, dominated by CEA |
CREST |
□ Conclusions
The incidence rate of carotid artery stenosis is also increasing in Korea. Among the patients with carotid artery stenosis, symptomatic carotid artery stenosis patient with higher risk of stroke (≥ 50% of stenosis) were selected as subjects for this study. The rate of death, stroke, myocardial infarction, and complications related with the CEA and CAS in patients with symptomatic carotid artery stenosis was compared by a systematic reviews and retrospective chart review. As a result, death and stroke in CEA was less occurred while complications were occurred more. As a result of cost-effectiveness analysis, the effectiveness difference of CEA and CAS was not that large, but CEA was less expensive than CAS, CEA was cost-effective option for carotid artery stenosis. To generalize these results to national level, the large-scale prospective, multicenter, randomized control trial should be conducted, and these comparative effectiveness research (CER) can provide the evidence of proper use of CEA and CAS.
|
Key Words: Carotid Artery Stenosis, Carotid Endarterectomy, Carotid Artery Stenting, Cost-benefit Analysis |
1. 서 론
1.1. 연구 배경
1.2. 연구의 필요성
1.3. 연구 목적
2. 선행연구
2.1. 경동맥 내막절제술과 스텐트 삽입술의 안전성 및 유효성
2.2. 경동맥 스텐트 삽입술과 내막절제술의 경제성 평가
2.3. 시술 현황
3. 유증상 경동맥 협착증 환자의 국내 시술 현황
3.1. 건강보험 청구자료 분석 방법
3.2. 건강보험 청구자료 분석 결과
4. 체계적 문헌고찰을 통한 스텐트 삽입술과 내막절제술의 안전성 및 유효성
4.1. 체계적 문헌고찰 연구방법
4.2. 체계적 문헌고찰 연구결과
5. 후향적 의무기록 조사를 통한 스텐트 삽입술과 내막절제술의 안전성 및 유효성
5.1. 후향적 의무기록조사 연구방법
5.2. 후향적 의무기록조사 연구결과
6. 경동맥 협착증의 삶의 질
6.1. 경동맥 협착증의 삶의 질 조사
6.2. 경동맥 협착증 치료 후 건강상태별 삶의 질
7. 경동맥 스텐트 삽입술과 내막절제술의 비용-효용분석
7.1. 분석개요
7.2. 분석모형
7.3. 효과 및 전이확률 추정
7.4. 효용 추정
7.5. 비용 추정
7.6. 기본분석
7.7. 불확실성 평가
8. 고찰
8.1. 연구결과 요약 및 고찰
8.2. 연구의 의의
8.3. 연구의 한계
8.4. 후속연구 제안
9. 결론 및 정책제언
10. 참고문헌
11. 부록
|



 연구정보
연구보고서
연구정보
연구보고서









 · 저작자표시
· 저작자표시 · 출처표시
· 출처표시



